
Publication Date:
January 2016 Vol. 11 No. 1
Author:
Kate Sheppard, PhD, RN, FNP, PMHNP-BC, FAANP
For many of us, nursing isn’t just what we do;
it’s who we are. Most of us became nurses because we care about people
and want to make a difference in their lives.
Over time, nurses develop a nursing intuition and a working
knowledge of disease and trauma. Our intuition, knowledge, and caring
don’t automatically shut off when we leave work. For example, have you
ever seen a worrisome mole on a complete stranger? Have you felt concern
about a friend’s weight or a neighbor’s smoking habits? Have you ever
been in a public place when you heard someone coughing—and wondered at
what point you might intervene? These experiences are common among
nurses. Yet, inability to shut off our knowledge and caring may leave us
feeling emotionally saturated and raise our risk for compassion
fatigue.
Ideally, as nurses, we should feel satisfied with our work and derive
satisfaction from providing excellent care. Compassion fatigue has been
defined as loss of satisfaction that comes from doing one’s job well,
or job-related distress that outweighs job satisfaction. Sometimes,
merely being exposed to another’s traumatic experience leaves us feeling
emotionally distraught. Called secondary traumatic stress, this is a
part of compassion fatigue. As our sense of job satisfaction decreases,
we may feel more burnout. A reaction to our work environment, burnout
can stem from such conditions as short-staffing, long work hours,
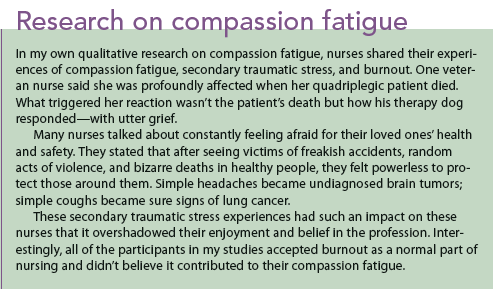
workplace incivility, and feeling dismissed or invalidated. (See
Research on compassion fatigue.)

Who gets compassion fatigue?
Compassion fatigue can happen to any nurse—and it can be
unpredictable. We know that nurses who work in oncology or see more
patient deaths may be at greater risk. Also, when we form close, caring
relationships with patients (especially if we lose our personal
boundaries), we may be putting ourselves at higher risk.
Sometimes a particular patient or a patient’s family member may
remind us of someone important in our lives. If that patient or family
member has died, we may be triggered emotionally. Many nurses I
interviewed in my research described being triggered unexpectedly and
profoundly by a smell (caring for a child with second- and third-degree
burns over 50% of his body), a sound (a mother screaming with grief when
told her 3-year-old child had coded and died), or a sight (a dog on the
hospital bed with his head across his master’s chest). Nurses who skip
breaks, take extra shifts, or come in on their days off out of a sense
of duty may be more at risk for compassion fatigue. One of the greatest
risks for compassion fatigue comes when nurses forgo their own
self-care.
What does compassion fatigue feel like?
In many cases, the first symptoms are emotional. Nurses talk about
feeling bored with their work or feeling detached and distant from
patients and colleagues. They may realize they’re irritable and
short-tempered. They may feel they’ve failed to relieve a patient’s pain
or to help a patient get well, losing their sense of pride in being a
nurse.
Frequently, nurses with compassion fatigue talk about sleepless
nights as they worry about what they forgot to do at work or replay
disturbing events in their minds. They may be forgetful at work, in
school, or at home. As compassion fatigue progresses, physical symptoms
typically arise. Most nurses describe feeling physically and mentally
exhausted, and many report headaches or backaches. Frequently, I hear
nurses say they feel queasy just driving to work, and those feelings
intensify as they walk in the door.
What happens to nurses who don’t deal with compassion fatigue
symptoms? First, their work performance changes; for example, they may
be at risk for medication errors. Without realizing why, they may start
to call in sick more frequently. They may be short-tempered, sarcastic,
or rude to colleagues and even to patients or families. They may appear
tired and may become more easily startled.
Unfortunately, they may attempt to reduce their emotional
saturation through alcohol or drug use. Ultimately, when emotional
saturation becomes too intense, some nurses may view leaving the
profession as the only means of escape.
Can you have compassion fatigue but still feel compassion?
Absolutely. In my studies, some nurses volunteered that they felt
symptoms of compassion fatigue, yet stated, “But I also still feel
compassion.” Clearly, a nurse can have symptoms of compassion fatigue
while still feeling compassion. If anything, the more compassion a nurse
feels, the greater the risk that she or he will experience emotional
saturation or compassion fatigue.
Reducing compassion fatigue
What can you do to reduce or even prevent compassion fatigue? Start
by being aware of how you feel physically and emotionally. If you
realize, for example, that interactions with a specific colleague often
feel uncomfortable or unpleasant, reflect on that a bit. Explore what’s
beneath that feeling.
Perhaps you feel overlooked, ignored, invalidated, unfairly
treated, or criticized—but instead of accepting those feelings and
trying to make a change, you compound your feelings with guilt and
shame. When you experience negative emotions, pay attention to how you
feel physically. By bringing physical and emotional feelings to the
surface, you can more efficiently address the underlying cause.
Establish healthy boundaries.
Establishing healthy boundaries is an important way to reduce the
risk of compassion fatigue. Many of us face minor boundary issues
frequently without really considering the consequences. Examples might
include answering a question you feel uncomfortable with, sharing
personal information you’d prefer to keep private, doing a favor for
someone not because you want to but because you feel you have to, having
someone hug or touch you in a way that makes you uncomfortable, and
tolerating a rude or pushy person. By slowing your response and doing
some self-reflection, you can address these issues with firm but
courteous responses.
Make self-care and self-compassion priorities.
Perhaps the most important way to prevent or reduce compassion
fatigue is to take care of yourself. As nurses, we work hard and really
need our breaks. We need to eat, and to take time for ourselves without
being interrupted by alarms, patients, or colleagues. We also need our
time off, for our mental and physical well-being.
Before you were a nursing student and nurse, you probably had
hobbies or activities you enjoyed. But later, between working long hours
and trying to balance your personal and professional lives, those
hobbies and activities were probably the first things you let go of. So
try to bring them back into your life. Take the dog for a walk every
day, listen to music, read a book for pleasure, go for a hike, call a
friend—do something for yourself every day.
Self-compassion is important, but it may be hard to attain. Start
noticing how you talk to yourself when frustrated, upset, or angry. Do
you berate or criticize yourself? Try replacing that talk with kindness,
just as you might talk to a loved one.
Practice self-reflection and mindfulness.
Parts of your job may make you feel frustrated because you feel
powerless. As burnout and compassion fatigue build, your emotions may
grow so strong that they become an overwhelming blur of anger,
resentment, frustration, or helplessness.
Thoughtful and quiet self-reflection away from work may help you
slowly separate events, interactions, and experiences. By examining each
event or interaction, you can become more aware of your triggers
(specific people, situations, or events) and address each one
individually. Even if you can’t change your work environment, you can
find power within by listening to your emotions with kindness and
approaching colleagues and others from a wise and centered perspective.
Mindfulness is an important part of self-compassion. Although
mindfulness has its roots in Buddhist meditation, it’s also a secular
cognitive practice in the form of mindfulness-based stress reduction.
To practice mindfulness, take note of the present and pay
attention with kindness and curiosity. You may notice physical or mental
feelings of pain, fatigue, or pleasure. If you feel pain, ask yourself
what your body or mind is trying to tell you—and address those concerns.
By engaging in mindfulness, you can learn to identify which areas of
your body react to your emotions. Mindfulness can reduce stress and
anxiety and improve your physical and mental well-being. Through
self-reflection and mindfulness, you allow yourself to consider events
and triggers, learn from them, forgive yourself, and move forward.
Taking action
We can all reduce our risk of compassion fatigue and emotional
saturation by reflecting on our triggers, practicing mindfulness,
replacing self-criticism with kind self-talk, and engaging in daily
self-care activities. Finally, if you’re suffering from sleeplessness,
poor self-care, loss of interest, or other symptoms of distress, reach
out for help from an employee assistance program or a mental health
provider.
Kate Sheppard is a clinical associate professor and the
psychiatric–mental health nurse practitioner specialty coordinator at
the University of Arizona College of Nursing in Tucson.
Selected references
Hinderer KA, VonRueden KT, Friedmann E, et al. Burnout,
compassion fatigue, compassion satisfaction, and secondary traumatic
stress in trauma nurses.
J Trauma Nurs. 2014;21(4):160-9.
Maiden J, Georges JM, Connelly CD. Moral distress, compassion
fatigue, and perceptions about medication errors in certified critical
care nurses.
Dimens Crit Care Nurs. 2011;30(6):339-45.
Neville K, Cole DA. The relationships among health promotion
behaviors, compassion fatigue, burnout, and compassion satisfaction in
nurses practicing in a community medical center.
J Nurs Adm. 2013;43(6):348-54.
Sheppard K. Compassion fatigue among registered nurses: connecting theory and research.
Appl Nurs Res. 2015;28(1):57-9.






 For
me, this past year has brought increased awareness of how quickly time
is passing and how easy it is to not make the most of the time we have. I
remember my beloved grandmother who firmly believed that taking time
for granted is an irreversible mistake. By the time we realize our
mistake, we find ourselves on the other side of an event that has
disrupted our foundations. Clearly, we cannot stop time or reverse
events that have already occurred.
For
me, this past year has brought increased awareness of how quickly time
is passing and how easy it is to not make the most of the time we have. I
remember my beloved grandmother who firmly believed that taking time
for granted is an irreversible mistake. By the time we realize our
mistake, we find ourselves on the other side of an event that has
disrupted our foundations. Clearly, we cannot stop time or reverse
events that have already occurred.