| The career handoff: Intentional sharing of knowledge and wisdom
Chapter from The Career Handoff, an STTI book.
|
| By Kathy Malloch and Tim Porter-O'Grady |
|
This chapter from The Career Handoff: A Healthcare Leader's Guide to Knowledge & Wisdom Transfer Across Generations examines the
critical components of successful communication, transition, handing
off, and succession planning in the healthcare profession.
“Tell me and I forget, teach me and I may remember, involve me and I learn.”
–Benjamin Franklin
 Every
year, Tim and I schedule time for a retreat to plan what we are going
to focus on in the next year. We select a special place where we can
both think and play and do something special. At our latest retreat at
the Ojai Valley Inn & Spa in California, we found ourselves
wondering how many more revisions of our work we could do—and how much
longer our ideas and strategies would be relevant for healthcare
organizations. And then came the even tougher question: What would
happen to our textbooks? Would Quantum Leadership just sail
into the sunset? We humbly wanted the information that would be
meaningful to future generations not to be lost; we did not want future
generations to rediscover what we had already identified and shared.
These questions got us to think about how to hand off our successful
ideas to younger colleagues and selectively discard that which is no
longer relevant. From that conversation, we began to strategize and
learn about how to hand off knowledge and wisdom to younger generations,
and this book is a result of those ideas. Every
year, Tim and I schedule time for a retreat to plan what we are going
to focus on in the next year. We select a special place where we can
both think and play and do something special. At our latest retreat at
the Ojai Valley Inn & Spa in California, we found ourselves
wondering how many more revisions of our work we could do—and how much
longer our ideas and strategies would be relevant for healthcare
organizations. And then came the even tougher question: What would
happen to our textbooks? Would Quantum Leadership just sail
into the sunset? We humbly wanted the information that would be
meaningful to future generations not to be lost; we did not want future
generations to rediscover what we had already identified and shared.
These questions got us to think about how to hand off our successful
ideas to younger colleagues and selectively discard that which is no
longer relevant. From that conversation, we began to strategize and
learn about how to hand off knowledge and wisdom to younger generations,
and this book is a result of those ideas.
We realized from our consulting practices that highly successful
professionals are often reluctant to consider retirement, and many
people avoid the thought of moving away from active engagement with
colleagues in sharing knowledge and wisdom. It is even more challenging
to figure out how to hand off or give one’s intellectual property to
another colleague. As an unprecedented number of baby boomers move
closer to retirement, there is much to share with succeeding
generations. There is also some content or intellectual property that
might not be applicable in future generations. We believe a formalized
process for sharing and designating intellectual property and products
would be helpful to not only our baby boomer colleagues but also to
other generations of colleagues.
The Need for Generational Sharing
Our professional consulting focus has been on the importance of leadership and in helping others to learn as much as possible about leadership—to embrace new ideas to become the most successful leaders possible. Our belief has always been that everyone is a leader, regardless of whether they have a formal leadership title. Whenever two individuals are together, one person begins the dialogue or movement in the simplest way, and leadership is evident. Each one of us has some special knowledge and expertise that future generations should or might want. Creating a culture as well as validating the science that assists others in handing off and nourishing our colleagues with our wisdom is important to both of us. Cultivating a culture of giving to others with minimal expectations of receiving something in return will allow future generations to grow and move on with what is vital to them. Our focus has shifted from figuring out what to give and how to instruct them to “love our stuff” to identifying interested colleagues and turning our work over to them to sort out and retain what is deemed valuable. It is also time for us to get out of the way of future leaders and shift from driving the boat to creating a safe space for others learning how to manage the boat’s journey!
Soon after our retreat, I was invited to keynote a leadership
summit group; my focus was on this topic of generational sharing.
Participants at this meeting included successful professionals from
three generations, including chief executive officers, nurse executives,
consultants, real estate executives, and physicians. As part of the
keynote, I presented the plan Tim and I developed to hand off two of our
books (see the feature that follows) and the discussion began to flow.
Participants were highly interested in learning more and becoming
involved in advancing the science of both giving and receiving
intellectual property and the wisdom of ages.
Reflecting on these ideas, we created a book proposal with the interested retreat participants. We now had a team of wisdom experts to join us on this journey and, most importantly, the authors represented three generations of interested professionals. We realized quickly that the importance of sharing generational wisdom was significant and that there was much interest from younger generations in learning more about our work and how to keep the useful knowledge alive and contemporary. Rather than seeing ourselves as the fading generation, it is time to see ourselves as a generation who now has much to share with the younger generations! We believe we created a talented team of wisdom managers to assist in this work.
Further dialogue with the contributing authors
provided clarification and enhancement of our ideas and solidified the
importance of documenting and sharing generational wisdom, successes,
and strategies that we would not repeat. We believe formalizing this
process and providing guidelines for colleagues will be an important
contribution to professional nursing practice. Each one of our authors
has included specific discussion on what the handoff is, some practical
tips for sharing knowledge, and exemplars to demonstrate personal
experiences (and, of course, some irreverent humor; we all need to laugh
and enjoy the nuances of our journey!).
This book reflects our commitment to professional
coaching, mentoring, and assuring that our young nurses are not chewed
up by the system but are supported proactively. Mentoring is a vital
professional behavior and an ethical obligation to our profession; we
need to nourish our young rather than engage in the proverbial “eating
our young.” In the next section, we share our personal and scholarly
connections to the art and science of mentoring.
Life Journey: Membership in the Profession
Transitions and transformations are a fundamental part of the journey of life. Naturally, as we age and grow, we gather information, skill, insight, and wisdom that accumulate and aggregate in a way that becomes a part of our characters and personalities. As professionals, one of the most important considerations is the responsibility that membership in the nursing profession brings. Who we are and what we are become a part of our professional identity such that our person and profession become one and the same thing (Malloch & Porter-O’Grady, 2010). As we journey through our careers and our lives and are recognized as professional nurses, we essentially become the “person of the nurse.” As professionals, we integrate our work, our relationships, and our individual persona in a way that creates the frame for who we are and provides the substance of the image we present to the world. Consider a notice you might see in a newspaper about the appointment of a position to an administrative or public role—the writer acknowledges the relationship between the person and profession by identifying the particular individual as a “physician.” However, when a nurse is appointed in a similar fashion to an administrative or public role, he or she will more frequently be identified as a “former nurse.” For the physician the identity is singular; for the nurse the same identity is dual (a nurse is a job different from the administrative or public role and, therefore, cannot be identified in singular terms).
“I am not a teacher, but an awakener.”
–Robert Frost
One of the joys of this life journey is the
increased knowledge, insight, and skill we develop as we aggregate
experiences and learning relationships. If we have had an open attitude
in all these arenas, we have been available to the opportunities to
deepen our insights and understandings and broaden our awareness in a
way that helps us develop expertise that advances our talent as
professionals. One of the urges this dynamic generates is the desire to
share and to extend these insights and talents in a way that benefits
others who are also eager for learning and personal development. This
desire to share knowledge and skill is an outgrowth of our own openness
and availability to learning and personal development. Those individuals
who understand this dynamic also recognize that embedded in it is the
give-and-take reflected in the interaction of all who share a commitment
to growing, learning, and deepening their knowledge and understanding.
|
Showing posts with label #nursestaffing. Show all posts
Showing posts with label #nursestaffing. Show all posts
Monday, June 13, 2016
Taking the Next Steps...Planned Succession
Monday, February 22, 2016
Nurse staffing and patient experience outcomes: A close connection
Focus on...Quality and Patient Safety
As healthcare providers set and refine their strategies for staying competitive in a value-based delivery and payment system, a sharper understanding of the interplay between inputs and outputs becomes a strategic imperative. Nurse staffing is a key input for acute-care hospitals—key both for its impact on care and its budget prominence. This puts it squarely at the center of hospitals’ efforts to deliver on their value promise.
The relationship between staffing and patient outcomes across quality, safety, and experience domains is appreciated intuitively, if not always precisely understood. The imperative to strike the perfect balance drives considerable interest and research in fine-tuning this understanding. Yet vast scholarship on the topic hasn’t produced a precise staffing formula that will lead predictably to desirable outcomes.
That’s because high-quality nursing care hinges on much more than the number of nurses on the job for a particular patient load. It also depends on multiple under-lying structural and process factors, such as nurses’ skills and education, availability of sufficient supplies and equipment, staff training, facilities, and reliable use of demonstrated best nursing practices—as well as such factors as interprofessional relationships, nurse engagement, and job satisfaction.
To fully understand the impact of staffing levels on patients’ clinical and experience outcomes, we must consider the relationships within and among these variables—something we can do only through data integration and cross-domain analytics.
Value of NDNQI data
In 2014, Press Ganey acquired the National Database of Nursing Quality Indicators® (NDNQI®)—the industry gold standard for assessing nursing excellence—from the American Nurses Association. NDNQI national benchmarking data are invaluable for monitoring key nursing-sensitive structure, process, and outcome measures. Similarly, Press Ganey’s vast patient experience database offers critical insight into patients’ perceptions about the effectiveness of hospital operations, clarity of the care team’s communication, and caregivers’ ability to meet patients’ needs.As with nurse staffing, a growing body of evidence shows associations between patient-experience outcomes and clinical outcomes. Combining NDNQI and patient-
experience data provides unprecedented access to the relationships among key pieces of information. Together, these measures can help nurse leaders identify how performance changes in certain structural and process indicators affect patient safety, experience, and clinical outcomes.
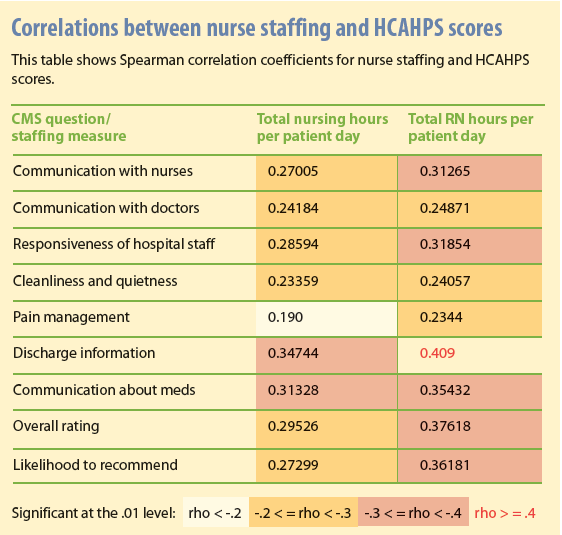
Given the enormous impact of nursing on the patient experience—and because nurse staffing often is a lightning rod in the debate on how to deliver high-value care—using the combined dataset to better understand how the two relate is a research priority. Our early analyses show that performance on both Press Ganey and Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) domains correlates significantly with nursing hours per patient day and RN hours per patient day, with the latter showing stronger associations in every domain. (See Correlations between nurse staffing and HCAHPS scores.) The link between more bedside nurses and a better patient experience isn’t surprising. That the correlations stretch across all experience domains—not just those that examine quality and frequency of nurse-patient interactions—is eye-opening.
Staffing that meets patient needs and reduces suffering
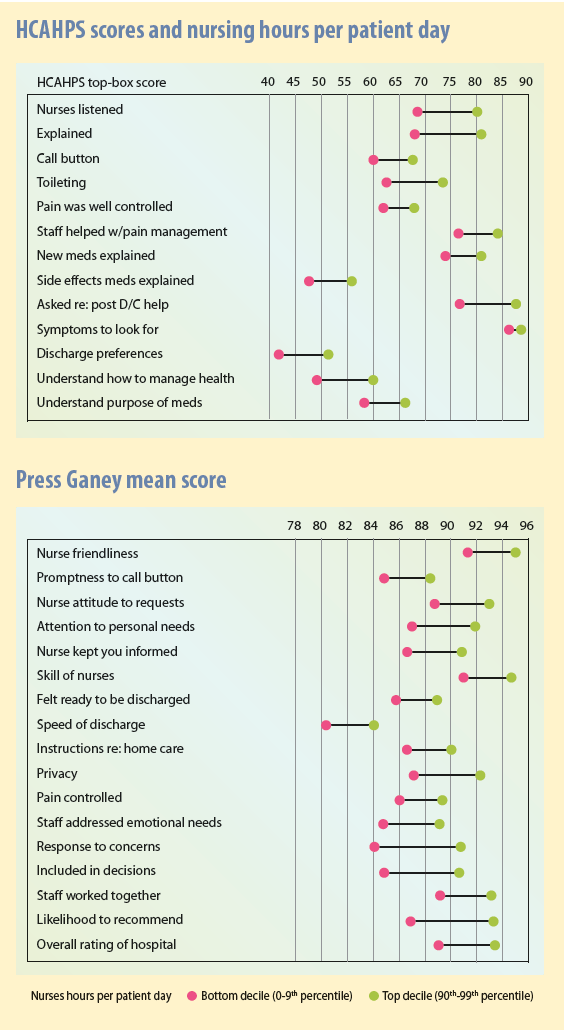
While domain-level correlations confirm long-held beliefs about the relationship between staffing and patient experience, we seek to understand which aspects of the patient experience are most sensitive to staffing. Where do staffing levels make a difference in caregivers’ success in meeting patient needs? Where can staffing serve as a lever to improve performance?Item- and question-level analyses help answer these questions. In the two tables HCAHPS scores and nursing hours per patient day and Press Ganey mean score, we see that for HCAHPS top-box scores and Press Ganey mean scores, every item showed sensitivity to staffing levels. Where the difference in patient experience scores is greatest (meaning when hospitals in the top decile of staffing ratios dramatically out-perform hospitals in the bottom decile), staffing can be viewed as a more powerful performance-improvement lever.
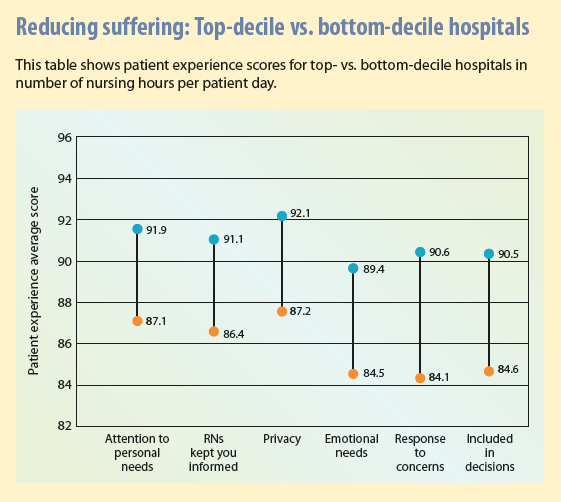
Reducing patient suffering
Of particular interest are differences in performance on key patient-experience questions related to patient suffering, which may indicate how effectively an organization provides patient-centered, personalized care. Press Ganey staff believe that relieving suffering should be central to efforts aimed at providing patient-centered care.Patient suffering falls into two categories:
- Inherent suffering results from the patient’s diagnosis, treatment, or both. It can’t be avoided entirely, but it can be mitigated. Some types of inherent suffering are well understood and addressed with some consistency—for instance, using pain control and explaining and managing symptoms. Inherent suffering includes psychosocial suffering, which caregivers are less comfortable with and therefore less practiced at addressing. Such suffering includes fear, anxiety, confusion, loss of dignity and autonomy, and uncertainty about self-care after discharge.
- Avoidable suffering arises from systemic defects, which may include long waits to receive treatment, poor communication, poor coordination among providers, errors, and failure to follow best practices. An important first step in determining how to avoid that kind of suffering is to understand that dysfunction creates additional suffering for people already burdened by inherent suffering.
It’s never just one thing
These findings don’t suggest that increasing nurse-patient ratios will automatically lead to performance improvements. Certainly, adequate nurse staffing is key to a range of outcomes, but changing staffing volume alone won’t produce optimal outcomes. Multiple aspects of structure and process also shape outcomes, and these findings must be leveraged with that in mind.Such factors as demographics of the nursing force, education and certification, engagement, and organizational staffing models are associated with patient-experience outcomes, as are cultural and structural practices and processes. In this regard, answers to the questions below also factor into outcomes:
- Is the nursing staff following best practices associated with better patient experiences?
- Are they executing on those best practices consistently and in the prescribed manner every single time?
- Do nurses have the right resources and training to promote consistency?
The concept of value over volume extends beyond changes to delivery and payment models. For hospitals, “getting it right” with their nursing organizations is particularly important because nursing care provides much of the value hospitals create. Adequate human resources are critical, but they’re not enough on their own. Nurse leaders must consider the full range of inputs—in addition to adequate human resources—that drive outcomes, including staff quality or caliber, the environment in which they operate, and shared commitment to providing a high-value experience for patients.
Nell Buhlman is senior vice president of Clinical and Quality Solutions at Press Ganey Associates in South Bend, Indiana. Note: Charts are copyrighted by Press Ganey and used with permission.
Selected references
Armstrong K, Laschinger H, Wong C. Workplace empowerment and Magnet hospital characteristics as predictors of patient safety climate. J Nurs Care Qual. 2009;24(1):55-62.
Dempsey C, Reilly B, Buhlman N. Improving the patient experience: real-world strategies for engaging nurses. J Nurs Adm. 2014; 44(3):142-51.
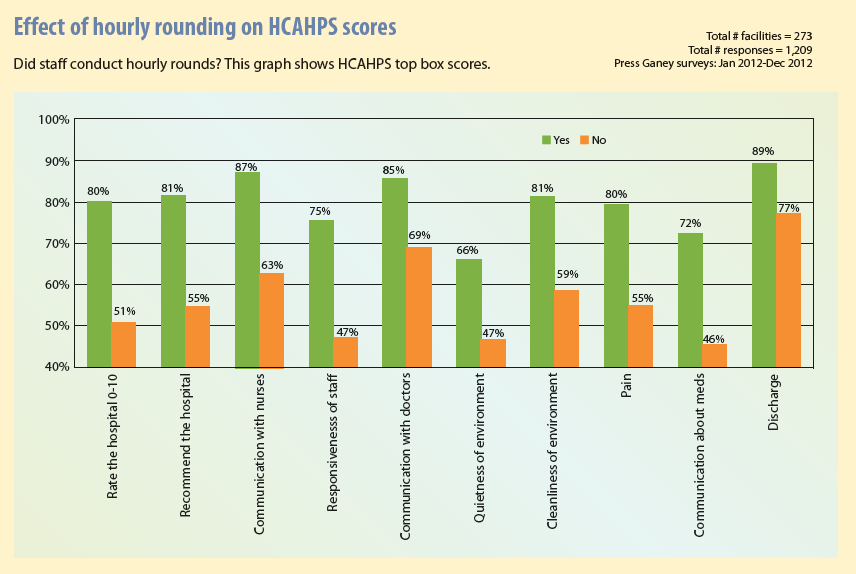
Halm MA. Hourly rounds: what does the evidence indicate? Am J Crit Care. 2009;18(6): 581-84.
Subscribe to:
Posts (Atom)