Publication Date:
Jan 2016 Vol. 11 No. 1
Author:
Fidelindo Lim, DNP, CCRN; Kimberly A. Weiss, MSN, FNP-BC; and Ingrid Herrera-Capoziello, MSN, RN, ANP NURSING
The transition from novice to expert nurse has
been an important topic in nursing circles for more than 30 years, since
Patricia Benner adapted the Dreyfus model of skills acquisition to the
nursing profession. The model still serves as an excellent conceptual
framework for the professional development of new nurses. Combined with
core competencies from the Quality & Safety Education for Nurses
(QSEN) initiative as the foundation for preceptor education, the model
provides a road map for assessing and evaluating skills acquisition of
new nurses or new preceptors. QSEN competencies include patient-centered
care, teamwork and collaboration, evidence-based practice, quality
improvement, safety, and informatics.
The impetus to anchor preceptor education to a solid framework
rests on evidence that prelicensure nursing education, although
sufficient for fostering formation of professional identity and ethical
comportment, doesn’t provide hands-on clinical experience. By focusing
on well-defined competencies such as those outlined in QSEN, preceptors
can better guide novice nurses on what skills to focus on and develop.
Preceptor council: Transforming education
Organizations with Magnet
® designation have vibrant,
robust unit practice councils that address such core safety issues as
falls, pressure ulcers, and hospital-acquired infections. At the
Hospital for Special Surgery in New York, NY, a robust preceptor council
composed of champions from all units and specialties grew out of a
staff-identified need. Co-chaired by two clinical nurse specialists and
overseen by the senior director of Nursing Excellence, the council meets
once a month to discuss challenges and opportunities for quality
improvement. It has become the forum for advocating transformational
preceptor education, leading to
a redesigned and interactive preceptor education model based on QSEN competencies.
Competency and life-experience osmosis
In the United States, the average age of the practicing nurse is near
50. Contrast this with 31—the average age of nurses graduating with
their initial nursing degree (considerably higher than the 1985 average
age of 24). Additionally, 52.8% of new RNs received a previous
bachelor’s degree and 7.2% hold a master’s degree or higher. The
implications of these evolving demographic trends vary and require
careful consideration when planning preceptor education. For example,
older students with higher qualifications may be more experienced and
have more confidence in addressing patient-care issues than traditional
nursing students. When planning preceptor education, the overall lived
experiences of new RNs must be taken into account.
Considering that preceptors generally are chosen from a pool of
more experienced senior nurses, the potential for transferring
hard-earned clinical skills and professional comportment is significant.
Failing to use this prolific source of human capital to the full
potential as knowledge, skills, and attitude transfer agents would
result in a great loss. Because a growing majority of new RNs are
entering nursing with professional backgrounds, they bring valuable and
diverse life experiences that can be harnessed to shape their
competencies in clinical judgment and technical proficiency.
Best practices for preceptor education
Situated learning, reflection on action, and outcomes measurement are
a few examples of evidence-based practices in high-quality preceptor
education.
Situated learning
Situated learning uses contextualized scenarios based on actual
events and demands of the nursing unit. Interactive exercises in small
group discussions using realistic and unfolding precepting case
scenarios engage would-be preceptors in situated learning, helping them
analyze and solve practice issues that might arise during preceptorship.
In this type of preceptor education, five carefully designed
scenarios dealing with such issues as generational differences,
experiential or learning gaps, missed opportunity, safety breaches, and
workaround and work ethic issues are appraised and critiqued. Learners
are asked to identify safety concerns, handle crucial conversations,
suggest a quality-improvement or a research project to address the
issues identified, and reflect on the merits of precepting best
practices. Learners then present their work to their peers and the
facilitator uses reflective questioning to address nuances of the
scenario.
Reflection on action
Reflection on action is a deliberate ongoing process of learning from
experience that will shape clinical judgment for future situations.
Because precepting is a high-stakes interface among staff members and
patients, it can cause significant stress. Effective preceptor education
should allow exploration of novel precepting challenges, either in
carefully designed scenarios or anecdotal reports from participants. The
goal of reflection on action is to highlight what preceptors gain from
their experience that contributed to their ongoing professional
development and to build capacity for clinical judgment in future
situations.
Outcomes measurement
The preceptor council’s deliberation at the Hospital for Special
Surgery conducted a pre- and post-training survey to assess how full-day
preceptor training was received and to appraise participants’ attitudes
toward precepting. Another survey was sent to trained preceptors after
they precepted a new staff member. Compared to pre-training survey data,
post-training data indicated an improved level of comfort and
confidence in precepting and an overwhelmingly positive attitude toward
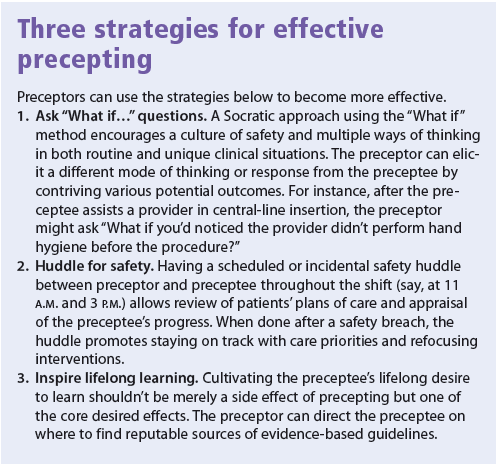
the preceptor role. (See
Three strategies for effective precepting.)

Preparing future preceptors
Seen through the lens of the QSEN competencies, preceptor education
prepares future preceptors not only as socializers of novice nurses into
the profession, but also as guardians of patient safety and quality
care. A conceptual or theoretical framework is an essential foundation
for a well-designed preceptor education. In organizations with Magnet
designation, creating a preceptor unit practice council fosters an
impetus to provide evidence on measurable outcomes.
Fidelindo Lim is an assistant clinical professor at New
York University College of Nursing in New York, N.Y. Kimberly A. Weiss
is a clinical nurse specialist in the postanesthesia care unit and
Ingrid Herrara-Capoziello is a clinical education specialist and
coordinator in the Office of Professional Development at the Hospital
for Special Surgery in New York, NY.
Selected references
American Nurses Association. Fast Facts. The Nursing Workforce 2014: Growth, Salaries, Education, Demographics & Trends.
http://goo.gl/uwHPH5
Benner P. From novice to expert.
Am J Nurs. 1982;82(3):402-7.
Benner P, Sutphen M, Leonard V, Day L.
Educating Nurses: A Call for Radical Transformation. San Francisco, CA: Jossey-Bass; 2010.
Budden JS, Zhong EH, Moulton P, Cimiotti JP. Highlights of the National Workforce Survey of Registered Nurses.
J Nurs Regulation. 2013:4(2):5-15.
Dreyfus SE, Dreyfus HL. A Five-Stage Model of the Mental
Activities Involved in Directed Skill Acquisition. ORC, 80-2, Operations
Research Center, University of California, Berkeley. 1980.
Ramsburg L, Childress R. An initial investigation of the
applicability of the Dreyfus skill acquisition model to the professional
development of nurse educators.
Nurs Educ Perspect. 2012;33(5):312-6.
Tanner CA. Thinking like a nurse: a research-based model of clinical judgment in nursing.
J Nurs Educ. 2006;45(6):204-11.
U.S. Department of Health and Human Services. Health Resources
and Services Administration. Bureau of Health Professions. National
Center for Health Workforce Analysis; April 2013. The U.S. Nursing
Workforce: Trends in Supply and Education.
http://goo.gl/ZjvLJs
U.S. Department of Health and Human Services. Health Resources
and Services Administration. The Registered Nurse Population: Findings
from the 2008 National Sample Survey of Registered Nurses. 2010.
http://goo.gl/1iyvPO